NAD+ Precursors and Cellular Aging: What Research Shows
**Meta Description:** Learn the truth about NAD+ precursors and cellular aging research—from clinical evidence to quality red flags. Discover what actually works for cellular health. --- You're scrolling through supplement ads at 11 PM, coffee g...

D.C.
Doctor of Chiropractic
Founder of FormulaForge. Doctor of Chiropractic revolutionizing nutritional supplements to be what we all wish they were — real quality, scientifically validated, with the exact ingredients and dosages we choose.
View Full ProfileReviewed by Dr. Brennan Commerford, DC
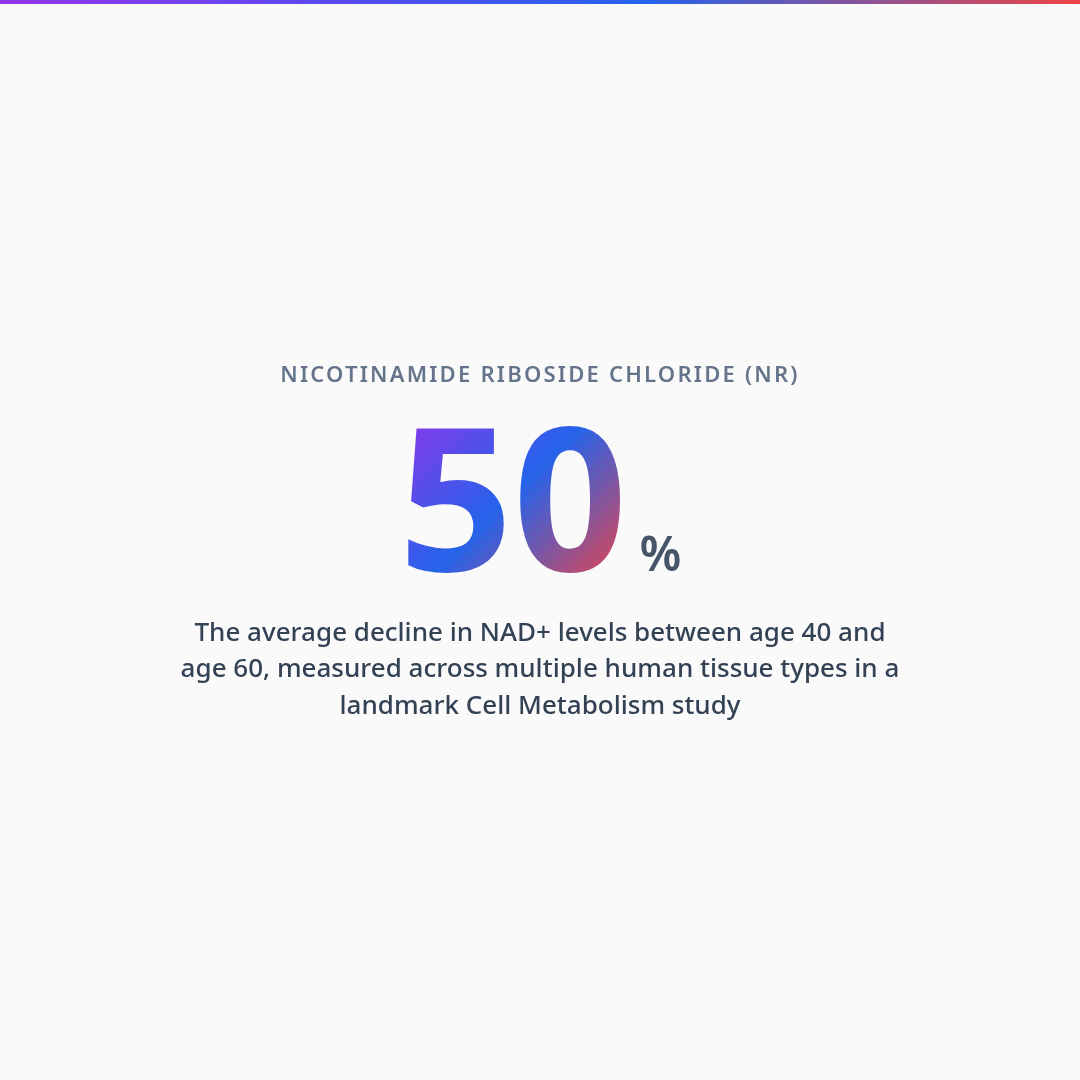
NAD+ declines roughly 50% between the ages of 40 and 60, affecting mitochondrial energy production, DNA repair, and sirtuin function — three systems directly implicated in how cells age. NMN and NR are the two most-studied precursors in human trials, and both raise circulating NAD+ levels. The clinical gap, however, is not whether to take a precursor. It is dose — most commercial products contain a fraction of the amounts used in published research. This guide explains the biochemistry, maps the precursor options, and identifies what to look for to determine whether a product will actually deliver a therapeutic dose.
The Molecule Everyone Is Buying and Few Are Dosing Correctly
NAD+ precursors have become one of the fastest-growing supplement categories in the longevity market. The science driving this interest is legitimate — NAD+ decline correlates with aging in reproducible, peer-reviewed human data, and precursor supplementation demonstrably raises circulating NAD+ levels in clinical trials. The problem is the gap between the clinical evidence and what most commercial products actually deliver.
In practice, patients came to me carrying bottles of NMN or NR that contained 50 to 100 mg per serving. The human trials showing meaningful outcomes used 250 to 1,000 mg daily. A patient spending forty dollars a month on a sub-therapeutic dose and reporting no benefit was not experiencing a failure of the science. They were experiencing a failure of product quality — which is not the same thing.
Understanding this distinction requires knowing what NAD+ actually does, how the precursors differ, and what constitutes a dose that the published research actually supports.
What NAD+ Does in the Cell
Nicotinamide adenine dinucleotide is not a supplement trend — it is a fundamental coenzyme present in every living cell, involved in hundreds of enzymatic reactions. Its most critical functions fall into three categories: energy production, genome maintenance, and cellular communication.
In mitochondria, NAD+ serves as the electron carrier that makes the electron transport chain functional. Without adequate NAD+, cells cannot efficiently convert glucose and fatty acids into ATP — the energy currency that powers contraction, cognition, healing, and every other active cellular process. When NAD+ is depleted, cellular energy production becomes inefficient and the consequences are felt systemically as fatigue, reduced exercise tolerance, and slower recovery.
For genome maintenance, the relevant enzymes are PARPs — poly ADP-ribose polymerases — which repair DNA strand breaks caused by normal metabolism, oxidative stress, and UV exposure. PARP activation consumes NAD+ at a rate that can substantially deplete cellular stores. When NAD+ is scarce, PARP activity slows, and unrepaired DNA damage accumulates. This is one of the proposed mechanisms linking NAD+ decline directly to aging biology rather than merely correlating with it.
For cellular communication, the relevant proteins are sirtuins — a family of seven enzymes that regulate gene expression, inflammation, stress resistance, and circadian rhythm. Sirtuins require NAD+ as a co-substrate to function. Low NAD+ means sirtuin activity is impaired across all seven members, with downstream effects on metabolism, inflammatory tone, and mitochondrial quality control.
NAD+ decline impairs three distinct systems simultaneously: energy production (mitochondria), genome maintenance (PARPs), and cellular regulation (sirtuins). These are not redundant systems — they interact. A cell with low NAD+ is energy-deficient, accumulating DNA damage, and running impaired regulatory programs at the same time.
The Decline Timeline Is Not Speculation
A 2016 study published in Cell Metabolism measured NAD+ levels in human tissue samples across age ranges from 20 to 80. The trajectory was consistent: approximately 20 to 25% decline by age 40, 40 to 50% decline by age 60, and levels in older adults that were a fraction of youthful baseline. This was not a single tissue finding — the decline was observed across skin, skeletal muscle, liver, and brain samples.
The research question this raises is whether the decline is a passive correlate of aging — a marker that something else is causing — or a mechanistic contributor. The evidence increasingly supports the mechanistic view. Studies in aged mice that restored NAD+ through precursor supplementation was associated with improvements in several age-related biomarkers in animal studies, including mitochondrial function, physical endurance, and inflammatory profiles. This does not prove that supplementing NAD+ precursors in humans will produce equivalent results — animal models are not direct translations — but it establishes a causal mechanism worth taking seriously.
A 2021 clinical trial published in Science gave healthy older adults NMN for 12 weeks at 250 mg daily. Researchers observed increased muscle NAD+ content, was associated with changes in metabolic markers in study participants, and enhanced aerobic capacity without significant adverse effects. A separate 2022 trial using nicotinamide riboside (NR) at 1,000 mg daily in older adults showed increased skeletal muscle NAD+ and was associated with changes in markers related to healthy immune response after six weeks. These studies are cited here not as definitive proof but as representative examples of the current human trial literature.
The Precursors: NMN vs. NR vs. Nicotinamide
NAD+ cannot be supplemented directly in meaningful amounts. The molecule is too large to cross cell membranes efficiently in oral form, and digestive enzymes break it down before it reaches circulation. Precursors work by providing smaller molecules the cell can absorb and convert into NAD+ through the intracellular salvage pathway.
NR is a form of vitamin B3 and the most-studied NAD+ precursor in human trials. A 2018 study found that 1,000 mg daily of NR increased blood NAD+ by approximately 60% in healthy adults, with the increase sustained throughout the supplementation period. Multiple subsequent trials confirmed this effect at doses ranging from 300 to 2,000 mg. NR is well-tolerated at clinical doses and does not produce the flushing associated with niacin.
NMN is one enzymatic step closer to NAD+ than NR, which has generated significant interest in whether it produces faster or more pronounced NAD+ elevation. Human studies are newer but growing. The 2021 trial in Science used 250 mg NMN daily and found increased muscle NAD+ content and improved metabolic markers. The absorption debate — whether NMN requires conversion to NR before cellular uptake or can be taken up directly via a specific intestinal transporter — has not fully resolved in the literature, but either mechanism results in NAD+ elevation. At present, both NMN and NR appear to be effective precursors; the evidence base for NR is more extensive, while NMN research is accumulating rapidly.
Nicotinamide does raise NAD+ levels through the salvage pathway, but it carries an important limitation at higher doses: it inhibits SIRT1 and other sirtuins — the same proteins that depend on NAD+ to regulate longevity-associated pathways. This creates a dose-dependent trade-off. At lower doses (under 500 mg daily), nicotinamide can maintain NAD+ levels without meaningful sirtuin inhibition and represents a cost-effective option for general maintenance. For patients whose primary goal involves sirtuin activation and the longevity-related signaling those enzymes support, NR or NMN are preferable.
The Dose Gap: Where Most Products Fail
This is the central quality issue in the NAD+ precursor market. Clinical trials demonstrating NAD+ elevation and associated metabolic effects use doses of 250 to 1,000 mg daily. A substantial proportion of commercial products — particularly those in the lower price range — contain 50 to 150 mg per serving. The disconnect is not marginal. A 100 mg dose of NR may produce some NAD+ elevation, but it is not the dose range that generated the clinical outcomes being cited in the product marketing.
Most NAD+ supplement marketing references clinical trial outcomes — improved mitochondrial function, was associated with changes in markers related to healthy immune response, enhanced metabolic parameters — that were achieved at doses of 250–1,000 mg daily. Many of the products cited alongside this research contain 50–150 mg per serving. The marketing references the science accurately; the dose does not match the evidence.
Check the Supplement Facts panel for the specific milligram amount of NR or NMN per serving. Then compare that number directly to the dose range used in the clinical trials cited on the label. If the product cites the REDUCE-IT equivalent for NAD+ research but delivers a quarter of the dose, you are paying for the branding, not the science.
A 2023 analysis of commercially available NAD+ precursor supplements found that the majority of products contained less than half the dose used in published clinical trials. Third-party testing also revealed that a significant proportion of products did not contain the form of compound listed on the label — receiving NR when the label says NMN, or vice versa. Form and dose verification via independent Certificates of Analysis is not optional in this category.
Supporting Co-Factors: What Helps NAD+ Work
NAD+ metabolism does not operate in isolation. Several co-factors are required for the enzymatic steps that convert precursors to NAD+ and for the downstream pathways those higher NAD+ levels are intended to support.
Riboflavin (vitamin B2) is a required co-factor for the enzyme that converts NR to NMN. Pyridoxine (vitamin B6) and other B vitamins participate in the broader NAD+ biosynthesis network. Magnesium is required for hundreds of enzymatic reactions including those in the sirtuin and PARP pathways. A patient optimizing for NAD+ pathway support on a background of suboptimal B vitamin or magnesium status may see attenuated response to precursor supplementation.
This is not an argument for buying every co-factor supplement on the market. It is an argument for ensuring that basic micronutrient status is not the limiting variable in a protocol designed to support NAD+ biology.
How FormulaForge Approaches NAD+ Precursor Classification
NAD+ precursors in the FormulaForge formulary are classified by precursor form (NR vs. NMN vs. nicotinamide), dose per serving relative to the clinical evidence range, and co-factor context. When you analyze a supplement label at myformulaforge.com, the system identifies whether your specific product is delivering a dose that falls within the published research range and whether your stack includes the B vitamins and minerals that support NAD+ pathway function. It also flags if multiple products in your stack contain overlapping precursors, which is relevant for total dose calculation when combining a dedicated NAD+ product with a multivitamin that includes niacin or nicotinamide.
Frequently Asked Questions
The science on NAD+ decline and precursor supplementation is real, peer-reviewed, and growing. Both NMN and NR demonstrably raise cellular NAD+ levels in humans at clinical doses. The problem is not whether the science supports supplementation — it is whether most commercial products are delivering a dose that the science actually supports. A 50 mg serving of NR is not the same as the 1,000 mg dose used in the trials being cited in its marketing. Verify the dose. Verify the form. Verify third-party testing. Then evaluate whether the product you are considering is built on the evidence or merely adjacent to it.
This article is intended for educational and informational purposes only and does not constitute medical advice. The information provided here is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or other qualified health provider with any questions you may have regarding a medical condition or supplement regimen. These statements have not been evaluated by the Food and Drug Administration. Dietary supplements are not intended to diagnose, treat, cure, or prevent any disease.
- Zhu XH, et al. In vivo NAD assay reveals the intracellular NAD contents and redox state in healthy human brain and their age dependences. Proc Natl Acad Sci USA. 2015;112(9):2876–2881.
- Camacho-Pereira J, et al. CD38 Dictates Age-Related NAD Decline and Mitochondrial Dysfunction through an SIRT3-Dependent Mechanism. Cell Metab. 2016;23(6):1127–1139.
- Trammell SA, et al. Nicotinamide riboside is uniquely and orally bioavailable in healthy humans. Nat Commun. 2016;7:12948.
- Elhassan YS, et al. Nicotinamide Riboside Augments the Aged Human Skeletal Muscle NAD+ Metabolome and Induces Transcriptomic and Anti-inflammatory Signatures. Cell Rep. 2019;28(7):1717–1728.
- Yoshino M, et al. Nicotinamide Mononucleotide Increases Muscle Insulin Sensitivity in Prediabetic Women. Science. 2021;372(6547):1224–1229.
- Igarashi M, et al. Chronic nicotinamide mononucleotide supplementation elevates blood nicotinamide adenine dinucleotide levels and alters muscle function in healthy older men. NPJ Aging. 2022;8(1):5.
- Bogan KL, Brenner C. Nicotinic acid, nicotinamide, and nicotinamide riboside: a molecular evaluation of NAD+ precursor vitamins in human nutrition. Annu Rev Nutr. 2008;28:115–130.
- Gomes AP, et al. Declining NAD+ Induces a Pseudohypoxic State Disrupting Nuclear-Mitochondrial Communication during Aging. Cell. 2013;155(7):1624–1638.